Medication Lung Risk Checker
Instructions: Select a medication you are taking or concerned about to view its specific risk profile and the critical symptoms to monitor. (Disclaimer: This is an educational tool, not a medical diagnosis. Always consult your doctor).
Select Medication
-
High RiskRisk Profile:
-
⚠️ Red Flags to Watch For:
| Key Point | Details |
|---|---|
| What it is | Lung scarring caused by specific medications, not by smoking or age alone. |
| Main Warning Signs | Dry cough, shortness of breath during exercise, and unexplained fever. |
| Critical Action | Stopping the drug immediately is the most effective way to prevent further damage. |
| Recovery Rate | 75-85% of patients recover well if the drug is stopped early. |
Which Medications Are the Biggest Culprits?
Not all drugs carry the same risk. Some cause a sudden, aggressive attack on the lungs, while others slowly build up damage over years. If you are taking any of the following, it is worth knowing the specific risks associated with them.First, let's look at Amiodarone, a common medication used for heart rhythm problems. It is notorious for pulmonary toxicity, affecting about 5-7% of long-term users. The damage usually happens after you've taken a cumulative dose of over 400 grams, often appearing 6 to 12 months into treatment. Because it's used for chronic heart issues, the lung damage can sneak up on patients who already have shortness of breath from heart failure.
Then there are the antibiotics. Nitrofurantoin, used for decades to treat urinary tract infections, is a frequent offender. Unlike heart meds, this one often affects elderly patients on long-term preventative therapy. Some people develop scarring after just six months, while others don't show symptoms for ten years. Because it's a "simple" antibiotic, many doctors and patients don't suspect it when a cough develops.
Chemotherapy drugs are among the most aggressive. Bleomycin is particularly high-risk, with 10-20% of patients experiencing lung toxicity. Other agents like Methotrexate-often used for rheumatoid arthritis-can cause acute pneumonitis, a rapid inflammation of the lungs, in about 1-7% of users. In recent years, newer cancer treatments called immune checkpoint inhibitors have also been linked to these scarring reactions, adding a new layer of complexity for oncologists.
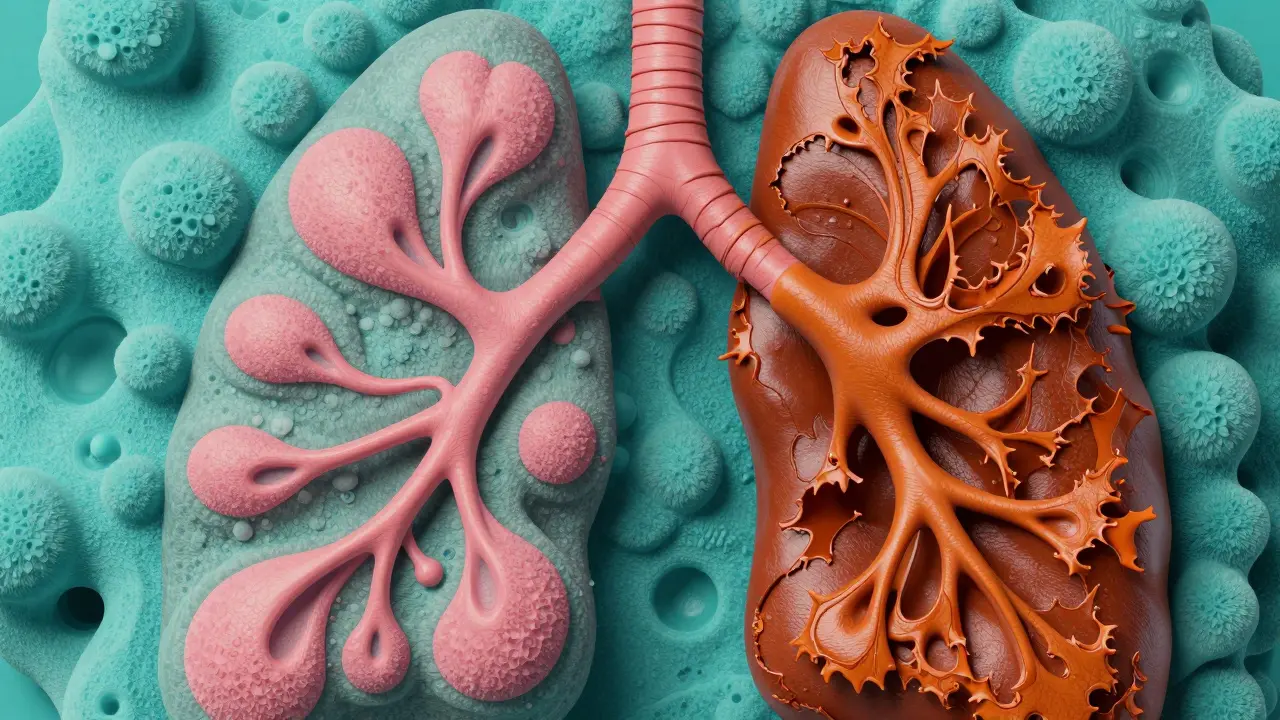
How the Scarring Actually Happens
You might wonder why a drug meant for the heart or a bladder infection would attack the lungs. The process usually starts with cellular damage. When these specific chemicals enter your system, they can create oxidative stress-essentially "rusting" the cells in your lung's air sacs (alveoli).Once the tissue is damaged, the body tries to heal itself. However, instead of replacing the cells perfectly, the body deposits Collagen, a tough protein that forms scar tissue. Imagine replacing a soft sponge with a piece of hard leather. The leather doesn't breathe; it doesn't expand. As more collagen builds up, the lungs become stiff, making it harder for oxygen to cross from the air sacs into your bloodstream.
This reaction is often idiosyncratic, meaning it doesn't follow a predictable pattern. Two people can take the exact same dose of a drug for the same amount of time, and only one will develop fibrosis. Researchers are currently hunting for genetic markers that might predict who is at risk, but for now, it remains a bit of a lottery.
Spotting the Red Flags
The biggest challenge with drug-induced lung disease is that the symptoms are generic. A dry cough or feeling winded after climbing a flight of stairs is often written off as "just getting older" or a side effect of the original illness. This leads to a dangerous diagnostic delay-on average, patients wait about eight weeks from the first symptom before the drug cause is identified.You should seek medical attention immediately if you notice these patterns:
- The "Exercise Gap": You used to be able to walk a mile, but now you're out of breath after half a block.
- The Persistent Dry Cough: A hacking cough that doesn't produce mucus and doesn't go away with over-the-counter syrups.
- Flu-like Symptoms: Unexplained low-grade fevers, fatigue, or joint pain accompanying your respiratory issues.
If you're on a high-risk medication, don't wait for these to become severe. Mention any new shortness of breath to your doctor immediately. Early detection is the only way to ensure the damage is reversible.
The Road to Recovery and Management
If a doctor suspects a medication is scarring your lungs, the first and most critical step is simple: stop the drug. This is the cornerstone of all treatment. In about 89% of cases, patients show improvement within three months just by removing the offending chemical from their system.However, stopping the drug isn't always enough if the inflammation is severe. Doctors often prescribe high-dose corticosteroids, such as Prednisone, to calm the immune system and stop the scarring process. This is usually tapered off over several months to avoid a relapse.
For those whose oxygen levels have dropped-specifically those with saturation below 88% at rest-supplemental oxygen therapy becomes necessary. This doesn't fix the scarring, but it protects the heart and brain from oxygen deprivation while the lungs attempt to heal.
Monitoring is a long-term commitment. You'll likely need spirometry (a breathing test) and diffusion capacity testing every few months. These tests measure how much air your lungs can hold and how efficiently oxygen is moving into your blood. While 75-85% of people make a good recovery, about 15-25% are left with permanent lung impairment, meaning they may need lifelong monitoring or oxygen support.

Preventing the Damage Before It Starts
We can't predict who will react poorly to a drug, but we can change how we monitor patients. There is a growing movement toward "baseline testing." This means getting a lung function test *before* you start a high-risk drug like amiodarone or methotrexate. If you have a baseline, your doctor can spot a 5% drop in lung function long before you actually feel short of breath.Communication is also key. Many patients aren't told that their medication carries a risk of lung scarring because doctors don't want to scare them. But knowing the risk is a tool for survival. When you start a new prescription, ask your provider: "Does this medication have a known risk for pulmonary toxicity, and what symptoms should I watch for?"
Can the lung scarring from drugs be completely reversed?
It depends on when the drug is stopped. If caught early during the inflammatory stage, much of the damage can be reversed. However, once actual collagen scarring (fibrosis) has set in, that tissue is generally permanent. The goal of treatment is to stop the progression and preserve the remaining healthy lung tissue.
Is the risk higher if I take the medication for a longer time?
For some drugs, yes. Amiodarone and Nitrofurantoin often show a correlation with long-term use or cumulative dosing. However, for other medications, the reaction can be idiosyncratic, meaning it can happen very quickly after the first few doses regardless of the total amount taken.
What tests do doctors use to diagnose drug-induced pulmonary fibrosis?
Diagnosis is a process of elimination. Doctors use High-Resolution CT (HRCT) scans to look for patterns of scarring and pulmonary function tests (PFTs) to measure lung capacity. Because there is no single "signature" look for drug-induced fibrosis, the most important piece of evidence is a detailed medication history.
Are there any alternatives to high-risk drugs that cause lung scarring?
Yes, depending on the condition. For example, if a patient cannot tolerate nitrofurantoin for UTIs, other antibiotics may be used. For heart rhythms, different anti-arrhythmic agents might be substituted. Always consult your doctor before switching medications, as the alternative must be equally effective for your specific health needs.
How common is this condition?
It is estimated to account for about 5-10% of all interstitial lung disease cases. While it is a small percentage of total lung diseases, the number of reported cases is rising as we develop more complex pharmaceutical therapies and improve our ability to detect the condition.
Next Steps for Patients and Caregivers
If you suspect you are experiencing side effects, the first step is to document your symptoms. Keep a daily log of when your cough worsens or when you feel most short of breath. This data is invaluable for your pulmonologist.If you are a caregiver, watch for "silent" symptoms. Older adults may not complain about breathlessness because they assume it's part of aging. Notice if they are taking more breaks while walking or if they are sleeping propped up on more pillows than usual to breathe easier. Prompt intervention can be the difference between a full recovery and permanent disability.




dallia alaba
April 20, 2026 AT 13:20It's really crucial to emphasize that the 'exercise gap' is often the first real sign. A lot of people just think they're out of shape, especially if they've been sedentary for a while. If you can suddenly not handle a walk to the mailbox, don't just shrug it off. Getting a baseline PFT before starting these meds is a game changer because you can't manage what you don't measure.
Lynn Smith
April 21, 2026 AT 03:56This is such helpful info! I'll definitely share this with my grandma, she's been on some of these for years and barely remembers the names of the meds.
Mike Beattie
April 21, 2026 AT 11:16The pathophysiology here is basically a textbook case of oxidative stress leading to aberrant fibroblast proliferation. If you aren't tracking your FVC and DLCO metrics, you're basically flying blind. Most GPs have zero clue about the nuanced differences between acute pneumonitis and chronic fibrotic remodeling. It's a systemic failure of primary care to not implement mandatory HRCT screening for high-risk cohorts.
Aaron McGrath
April 22, 2026 AT 15:25STOP WAITING AROUND! If you're feeling winded, get your ass to a pulmonologist NOW! This isn't some 'maybe later' situation. The window for reversing that inflammation is tiny before it turns into permanent leather in your chest. Use the data, push your doctor for a baseline test, and don't let some generic 'you're just aging' excuse ruin your life! MOVE FAST!
Arthur Luke
April 24, 2026 AT 03:29I wonder if the prevalence is higher in certain populations based on diet or other environmental factors that might exacerbate the oxidative stress mentioned.
julya tassi
April 24, 2026 AT 21:19This is actually kind of terrifying but so important to know! 😱 I had no idea a simple UTI drug could do this. Definitely adding 'ask about lung risk' to my list for my next checkup! Thanks for sharing! 😊
Brigid Prosser
April 25, 2026 AT 16:32Listen up, if you're caring for an elderly parent, be the voice they don't have. They'll tell you they're 'just tired' while they're actually struggling for every breath. Grab them by the hand and get them to a specialist. It's an uphill battle sometimes, but catching this early is the only way to keep them out of an oxygen tank. Stay sharp and be assertive with the medical staff!
Akshata Kembhavi
April 25, 2026 AT 21:22Really interesting read. I've seen a few people in my community struggle with chronic coughs and they never even thought about their heart meds being the cause.
Lucy Kuo
April 26, 2026 AT 23:23It is truly heartbreaking to contemplate the sheer devastation that an unsuspecting patient must feel when a remedy for a minor ailment transforms into a lifelong respiratory struggle. The notion of our vital organs becoming as stiff as leather is an image of profound tragedy. We must advocate for a more transparent dialogue between physicians and patients to ensure such calamities are averted through early vigilance and compassionate care. One cannot overstate the necessity of baseline testing in our modern pharmaceutical landscape.
Grace Grace
April 27, 2026 AT 18:25Oh my goodness, this is so scary!! I laways thought meds were safe if the doctor presribed them!! We need to be so much more carefull about these side effects befor they become permanant!!!
Charlotte Boychuk
April 28, 2026 AT 12:34Just a little reminder to everyone to keep it chill while talking to your docs. No need to go in there swinging, just a little curious conversation about the side effects can save you a world of trouble. It's all about that balance between trusting the medicine and keeping your eyes open. Let's just keep supporting each other through the health scares.
caesar simpkins
April 29, 2026 AT 16:48It's a heavy realization that the very tools we use to heal can sometimes leave a permanent scar on our lives. The imagery of the sponge turning to leather is just... vivid. It really puts the urgency into perspective. Just take a deep breath-while you still can-and make sure your loved ones are getting the tests they need. It's a lot to process, but knowing is half the battle.