
Why Opioid Constipation Is More Than Just a Nuisance
If you’re taking opioids for chronic pain, cancer, or after surgery, you’ve probably heard that constipation is a common side effect. But calling it just a nuisance undersells how serious it is. Up to 80% of people on long-term opioids develop opioid-induced constipation (OIC), and for many, it’s so bad they stop taking their pain meds altogether. Unlike regular constipation, OIC doesn’t respond well to fiber, water, or over-the-counter laxatives. Studies show less than 30% of chronic users get relief from traditional treatments. That’s because opioids don’t just slow things down-they lock up the natural movement of your gut by binding to mu-opioid receptors in the intestinal wall. These receptors control how fast food moves, how much fluid is absorbed, and whether your bowels feel the urge to go. Block those receptors, and your digestive system essentially goes on pause.
What Are Peripherally Acting Mu Antagonists (PAMORAs)?
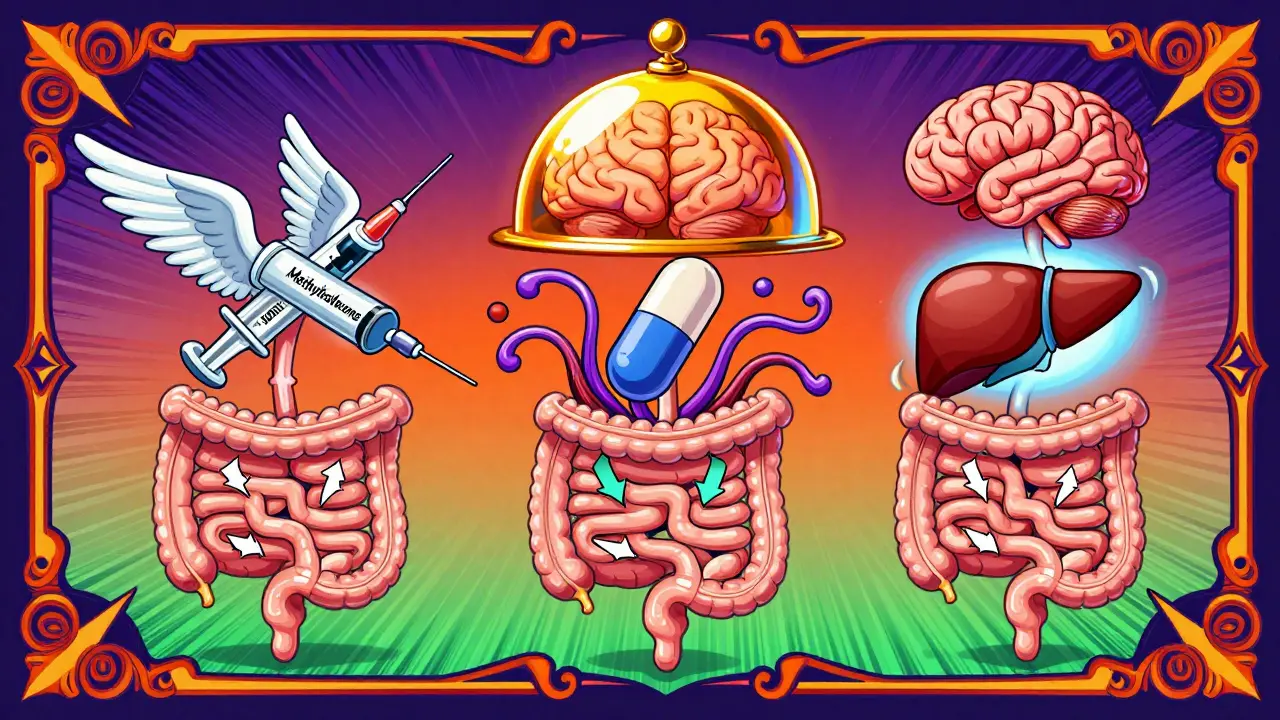
PAMORAs are a class of drugs built to fix this problem without touching your pain relief. Unlike regular opioid blockers like naloxone, which can reverse pain control by crossing into the brain, PAMORAs are designed to stay outside the central nervous system. They block opioid receptors in the gut but can’t cross the blood-brain barrier in meaningful amounts. That means your pain stays managed, but your bowels start moving again. The first PAMORA approved by the FDA was methylnaltrexone in 2008, followed by alvimopan and later naloxegol and naldemedine. Each one works the same way but has different chemical tweaks to improve how long it lasts, how it’s taken, and who it’s safe for.
The Three Main PAMORAs You Need to Know
There are three primary PAMORAs used today, each with unique features:
- Methylnaltrexone (RELISTOR): This is a quaternary amine with a molecular weight of 429.32 g/mol. Because it’s charged, it can’t easily pass into the brain. It’s available as a subcutaneous injection (0.15 mg/kg) or an oral tablet (450 mg). It works fast-most people have a bowel movement within 4 hours. It doesn’t interact with liver enzymes like CYP3A4, so it’s safe to use with many other drugs. It’s the only PAMORA approved for both cancer patients in palliative care and those with chronic noncancer pain.
- Naloxegol (MOVANTIK): This is a modified version of naloxone with a polyethylene glycol chain attached, making it too big to enter the brain easily. Taken as a 25 mg daily tablet, it reaches peak levels in about 2.5 hours and lasts 8-13 hours. It’s not recommended for people with severe kidney problems or moderate liver impairment. In clinical trials, about 44% of patients had a spontaneous bowel movement within 12 weeks, compared to 30% on placebo.
- Naldemedine (SYMPROIC): Also an oral tablet (0.2 mg daily), naldemedine uses a similar polyethylene glycol trick to stay out of the brain. It’s been shown to help 48% of patients have regular bowel movements, versus 35% on placebo. It’s cleared through the liver, so it needs caution in people with moderate to severe liver disease. Unlike naloxegol, it doesn’t require dose adjustments for kidney issues.
How Effective Are They Really?
Real-world results vary, but the data is clear: PAMORAs work better than anything else for OIC. In one trial with 330 patients, 52% of those on methylnaltrexone had a bowel movement within 4 hours, compared to just 30% on placebo. Naloxegol and naldemedine showed similar results over 12 weeks, with response rates hovering around 45-48%. That’s a big jump from the 20-30% you get with laxatives. But effectiveness isn’t just about numbers. Many patients report being able to eat normally again, sleep better, and stop dreading daily bowel struggles. On patient forums, people with cancer on palliative care often say methylnaltrexone changed their lives. One Reddit user wrote, “I finally stopped worrying about being stuck for days. I could go out with my family again.”
Where They Fall Short
They’re not perfect. About one in three patients report abdominal cramping or nausea, especially when starting treatment. Some people find the effects fade over time-like one 67-year-old with osteoarthritis who told Healthgrades, “It worked for two weeks, then stopped. I paid $450 a month for nothing.” Others say the cost is a dealbreaker. Without insurance, a year’s supply of any PAMORA can run $5,000-$6,000. Even with coupons, out-of-pocket costs can hit $200-$400 a month. That’s why many patients never start them. Also, they’re useless if you have a physical blockage in your intestines. All labels warn against use in cases of mechanical obstruction. And while early concerns about PAMORAs triggering pain flare-ups turned out to be exaggerated, a small number of sensitive patients still report increased discomfort.

How to Use Them Right
Getting the most out of a PAMORA isn’t just about picking the right one-it’s about timing and dosing. Most doctors underdose at first. A 2022 survey of 250 pain specialists found 78% started too low. The key is to match the PAMORA’s peak action with your opioid’s peak effect. If you take oxycodone at 8 a.m. and 8 p.m., and it hits its highest level around 11 a.m. and 11 p.m., take the PAMORA at 10 a.m. and 10 p.m. That way, it’s blocking the gut receptors just as the opioid is trying to slow things down. For methylnaltrexone injections, the first dose is usually given in a clinic. After that, patients can self-administer. Oral versions can be started at home. Always check kidney and liver function before starting-naloxegol is risky if your kidneys are weak, and naldemedine needs caution with liver disease. Dose adjustments are critical.
Market Trends and Future Outlook
PAMORAs are a growing part of the $2.8 billion opioid constipation market, projected to hit $4.1 billion by 2027. Methylnaltrexone still leads with 45% of sales, followed by naloxegol and naldemedine. But change is coming. In January 2023, a new 300 mg methylnaltrexone tablet was approved for patients who don’t respond to the standard dose. The NIH is testing a combo drug that pairs a PAMORA with a serotonin agonist-early results show a 68% response rate. Meanwhile, the first methylnaltrexone biosimilar is in phase 3 trials in China. Still, access remains limited. The American Gastroenterological Association warns that without price drops, only 35-40% of eligible patients will ever get them. For now, PAMORAs remain the gold standard-not because they’re cheap or perfect, but because they’re the only drugs that treat the root cause, not just the symptoms.
What Comes Next?
If you’ve tried laxatives, stool softeners, and enemas without success, PAMORAs are worth discussing with your doctor. They’re not a first-line fix, but for people who’ve hit a wall with standard care, they offer real relief. The biggest barrier isn’t science-it’s cost and awareness. Many patients don’t even know these drugs exist. If you’re on opioids and struggling with constipation, ask: “Is a PAMORA right for me?” Don’t wait until you’re ready to quit your pain meds. There’s a targeted solution that keeps your pain under control while getting your bowels moving again.
Can PAMORAs reverse opioid pain relief?
No. PAMORAs are designed to act only in the gastrointestinal tract and don’t cross the blood-brain barrier in significant amounts. Clinical trials confirm they preserve opioid pain control while improving bowel function. Studies show no meaningful reduction in analgesic effectiveness at standard doses.
Are PAMORAs safe for cancer patients?
Yes. Methylnaltrexone is specifically approved for cancer patients in palliative care and has been shown to improve quality of life without interfering with pain management. Many patients in hospice and oncology settings rely on it to maintain comfort and dignity.
How quickly do PAMORAs work?
Methylnaltrexone injection works fastest-about 50% of patients have a bowel movement within 4 hours. Oral forms like naloxegol and naldemedine take longer, with effects building over days to weeks. Most patients see improvement within the first week, but full benefit may take up to 12 weeks.
Can I take a PAMORA with other laxatives?
Yes, but it’s usually not necessary. PAMORAs are more effective than traditional laxatives for opioid constipation. If you’re still having trouble after starting a PAMORA, your doctor may add a mild osmotic laxative like polyethylene glycol, but combining multiple strong stimulants increases the risk of cramping and dehydration.
Why is alvimopan not used for chronic opioid constipation?
Alvimopan was approved only for short-term use after bowel surgery to speed up recovery. Long-term use was linked to increased risk of heart attack in clinical trials. Because of this, it’s restricted to hospital use under a special safety program and is not approved for ongoing opioid constipation.



Bryan Coleman
January 31, 2026 AT 12:44Still can’t believe it took my pain doc 3 years to mention it.
franklin hillary
February 1, 2026 AT 13:05PAMORAs are literally magic for the gut
Why aren’t these in every pain clinic yet
Someone’s making bank keeping people miserable with Miralax and hope
Bob Cohen
February 1, 2026 AT 17:52Just saying. Maybe we should be asking why we’re prescribing so much in the first place.
Ishmael brown
February 3, 2026 AT 09:42Worth $400 a month? Nah. I’d rather eat prunes and pray.
Aditya Gupta
February 4, 2026 AT 22:00Nancy Nino
February 5, 2026 AT 20:13June Richards
February 7, 2026 AT 09:00Maybe if you ate a vegetable once in a while you wouldn’t need this nonsense.
Jaden Green
February 8, 2026 AT 10:43Lu Gao
February 9, 2026 AT 06:27Also, the 68% response rate with the new combo drug? That’s wild. Can’t wait to see phase 3 results.
Angel Fitzpatrick
February 9, 2026 AT 10:48Nidhi Rajpara
February 10, 2026 AT 06:21Chris & Kara Cutler
February 10, 2026 AT 16:40