Did you know that taking a standard dose of painkillers or blood pressure medicine can hit an 80-year-old body like a double dose? It sounds scary, but it’s the biological reality for millions of seniors. As we age, our internal organs don't just slow down; they change structure. The liver and kidneys, which act as the body's filtration and processing plants, lose efficiency. This isn't about getting 'old'-it's about specific physiological shifts that alter how drugs are absorbed, processed, and eliminated.
If you're caring for an older adult, or if you are one, understanding these changes is the difference between effective treatment and a trip to the emergency room. Adverse drug reactions account for roughly 10% of hospital admissions in elderly patients. That’s not a small number. Let’s break down exactly what happens inside the body and how to manage medications safely.
The Silent Shifts in Liver Function
The liver is the primary engine for metabolizing most medications. In young adults, this organ is robust, with high blood flow and massive enzymatic activity. But by the time someone reaches their 70s or 80s, the landscape has changed significantly.
First, there is less liver tissue. Research shows that liver mass decreases by approximately 30% in older adults compared to younger individuals. Think of it like a factory closing down several assembly lines. There are simply fewer cells available to process incoming chemicals.
Second, and perhaps more critically, blood flow to the liver drops. Hepatic blood flow can decrease by up to 40%. This matters because many drugs rely on being carried to the liver by the bloodstream to be broken down. When traffic slows down, the cars (the drugs) pile up.
| Physiological Factor | Change in Older Adults | Clinical Consequence |
|---|---|---|
| Liver Mass | Reduces by ~30% | Fewer enzymes available to break down drugs |
| Hepatic Blood Flow | Decreases by ~40% | Slower delivery of drugs to metabolic sites |
| Phase I Enzyme Activity | Variable decline (up to 60% in some models) | Prolonged effect of certain sedatives and anesthetics |
| Phase II Enzyme Activity | Relatively preserved | Some drugs remain stable despite age |
This reduction in blood flow specifically impacts "flow-limited" drugs. These are medications that the liver clears very efficiently when blood flow is normal. Examples include propranolol (a beta-blocker), lidocaine (an anesthetic), and morphine. Because the liver extracts so much of these drugs from the blood passing through it, a drop in blood flow means less drug gets processed. The result? Higher levels of the drug stay in the bloodstream longer, increasing the risk of side effects like dizziness, confusion, or respiratory depression.
Kidney Decline: The Hidden Risk
While the liver processes drugs, the kidneys excrete them. Age-related kidney changes are often more predictable than liver changes, yet they are frequently overlooked in clinical practice.
The key metric here is the Glomerular Filtration Rate (GFR). GFR measures how well your kidneys filter waste from the blood. Between ages 30 and 80, GFR typically declines by 30-50%. However, here is the trap: serum creatinine levels-a common marker used to estimate kidney function-often remain stable in older adults. Why? Because muscle mass decreases with age. Since creatinine is a byproduct of muscle breakdown, less muscle means less creatinine produced, even if the kidneys are filtering poorly.
This creates a dangerous illusion. A doctor might look at a normal creatinine level and assume kidney function is fine. In reality, the GFR could be dangerously low. If a patient is prescribed a renally cleared drug like gabapentin (for nerve pain) or certain antibiotics without adjusting for this hidden decline, the drug accumulates. This can lead to toxicity, severe sedation, or further kidney damage.
To get an accurate picture, clinicians use equations like the Cockcroft-Gault equation or the newer CKD-EPI equation. These formulas factor in age, weight, and gender to estimate true kidney function, bypassing the misleading stability of raw creatinine numbers.
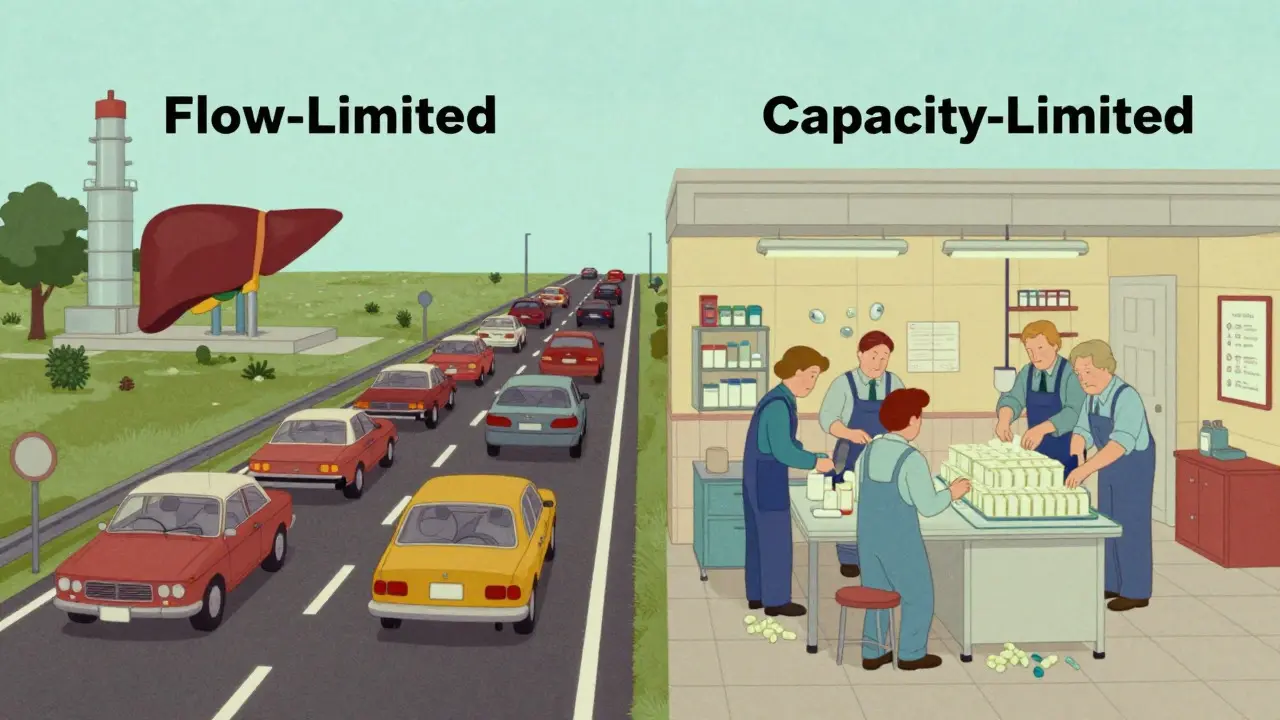
Flow-Limited vs. Capacity-Limited Drugs
Not all drugs react the same way to aging organs. Pharmacologists categorize drugs based on how they are cleared: either by blood flow (flow-limited) or by enzyme capacity (capacity-limited).
- Flow-Limited Drugs: As mentioned, these have a high hepatic extraction ratio (>0.7). Their clearance is directly tied to liver blood flow. Since blood flow drops significantly with age, clearance drops too. You need lower doses of these drugs in older adults. Examples: Morphine, Propranolol, Verapamil.
- Capacity-Limited Drugs: These have a low hepatic extraction ratio (<0.3). Their clearance depends on the amount of enzyme present, not how fast blood flows. Since liver enzyme content remains relatively preserved in many older adults, clearance for these drugs doesn't change as drastically. However, individual variability is high. Examples: Diazepam, Phenytoin, Theophylline.
There is also a third category: prodrugs. These are inactive substances that the liver must convert into active medicine. Perindopril, an ACE inhibitor for blood pressure, is a prodrug. If the liver's conversion ability slows down due to age, the patient might not get enough active drug, leading to uncontrolled blood pressure. This is the opposite problem-under-dosing rather than over-dosing.
The Polypharmacy Trap
Aging organs are bad enough on their own. Add polypharmacy-the concurrent use of five or more medications-and the risk skyrockets. Data from the National Health and Nutrition Examination Survey (NHANES) shows that 41% of adults aged 65+ use five or more prescription meds.
When multiple drugs compete for the same liver enzymes (like Cytochrome P450), they can block each other's metabolism. One drug stays in the system longer, amplifying its effects and side effects. This is known as a drug-drug interaction. For example, combining a statin (cholesterol med) with a macrolide antibiotic can inhibit the enzyme that breaks down the statin, leading to muscle toxicity.
In older adults, where the liver and kidneys are already working at reduced capacity, these interactions are more likely to cause harm. The margin for error shrinks. A slight increase in drug concentration that a 30-year-old wouldn't notice might cause a fall or a stroke in an 80-year-old.

Practical Steps for Safer Medication Management
So, what can you do? Whether you are a caregiver, a family member, or managing your own health, here are actionable steps to mitigate risks.
- Start Low, Go Slow: This is the golden rule of geriatric prescribing. Initial doses should often be 20-40% lower than standard adult doses. Titrate up slowly only if necessary and tolerated.
- Regular Medication Reviews: Don't wait for annual checkups. Review all medications-including over-the-counter drugs and supplements-at least twice a year. Ask: "Is this still needed? Can we reduce the dose?"
- Monitor Renal Function Properly: Ensure your doctor is calculating eGFR (estimated Glomerular Filtration Rate) using age-appropriate formulas, not just looking at creatinine. Request a copy of these results.
- Use Screening Tools: Doctors can use tools like the Beers Criteria® or STOPP/START criteria to identify potentially inappropriate prescriptions for older adults. Ask if your medications pass these screens.
- Watch for Subtle Signs: Side effects in older adults often manifest as confusion, dizziness, falls, or loss of appetite, rather than classic symptoms like nausea or rash. Report these changes immediately.
Technology is also helping. New pharmacokinetic modeling software allows clinicians to simulate how a specific patient's age, weight, and organ function will affect drug levels. While not yet universal, this represents a move toward precision geriatric pharmacology.
Conclusion: Proactive Care Saves Lives
The changes in liver and kidney function during aging are inevitable, but adverse drug events are not. By recognizing that the body's processing power diminishes, we can adjust our approach to medication. It requires vigilance, regular monitoring, and open communication with healthcare providers. The goal is not to avoid medication, but to use it smarter, safer, and more effectively for the unique physiology of older adults.
Why do older adults need lower doses of medication?
Older adults experience a natural decline in liver mass (by ~30%) and hepatic blood flow (by ~40%), as well as a significant drop in kidney filtration rate (GFR). This means drugs stay in the body longer and at higher concentrations. Lower doses prevent toxicity and severe side effects.
What is the difference between flow-limited and capacity-limited drugs?
Flow-limited drugs (like morphine) are cleared primarily by blood flow to the liver. Since blood flow decreases with age, these drugs accumulate easily. Capacity-limited drugs (like diazepam) depend on enzyme amounts, which remain relatively stable, so their clearance is less affected by age-related blood flow changes.
Why is serum creatinine an unreliable indicator of kidney function in seniors?
Serum creatinine comes from muscle breakdown. Older adults often have less muscle mass, so they produce less creatinine. This can make kidney function appear normal in blood tests even when the Glomerular Filtration Rate (GFR) has actually declined significantly. Doctors should use calculated eGFR instead.
How does polypharmacy increase risk in older adults?
Polypharmacy involves taking multiple medications simultaneously. In older adults with reduced liver and kidney function, these drugs can interact, competing for the same metabolic pathways. This leads to unpredictable drug levels, increasing the likelihood of adverse reactions, falls, and hospitalizations.
What are the Beers Criteria?
The Beers Criteria is a widely used guideline developed by the American Geriatrics Society. It lists medications that are potentially inappropriate for older adults due to increased risks of side effects or lack of efficacy. It helps doctors avoid prescribing drugs that pose unnecessary dangers to seniors.