When someone turns 70, they might be taking five, ten, or even fifteen different pills every day. Some for blood pressure. Others for diabetes, arthritis, sleep, or heart rhythm. It’s not unusual. But it’s dangerous. Polypharmacy-the use of five or more medications at once-is now the norm for millions of older adults, and it’s quietly putting lives at risk.
What Exactly Is Polypharmacy?
Polypharmacy isn’t just about taking a lot of pills. It’s about taking the wrong ones, at the wrong times, for the wrong reasons. The standard definition? Five or more medications daily. But experts now warn that even three or four can be risky if they interact poorly. The real problem? Many of these drugs aren’t necessary anymore-or they’re causing more harm than good.By 2020, over 15% of the global population was 65 or older. By 2060, that number will jump to nearly 44%. With aging comes chronic illness: heart disease, diabetes, arthritis, dementia. Each condition often brings its own prescription. Doctors don’t always talk to each other. So a patient might get a statin from their cardiologist, a painkiller from their orthopedist, an antidepressant from their psychiatrist, and a sleep aid from their primary care doctor-all without anyone checking if they clash.
Studies show that 40% of older adults globally are on five or more medications. In U.S. physician offices, that number hits 65%. Among nursing home residents? Over 80%. And it’s rising. From 2010 to 2019, the percentage of older adults on ten or more drugs jumped from 10% to 14%. That’s not progress. That’s a crisis.
Why Do These Medications Become Dangerous?
Your body changes as you age. Your kidneys don’t filter as well. Your liver doesn’t break down drugs the same way. Your brain becomes more sensitive to sedatives. Even small doses can cause dizziness, confusion, or falls. And with each new pill you add, the risk of a bad interaction explodes.Take two medications: there’s a 6% chance they’ll interact. Add three more? That jumps to 50%. With seven or more? You’re almost guaranteed a problem. These aren’t theoretical risks. They’re happening in real homes, in real ERs.
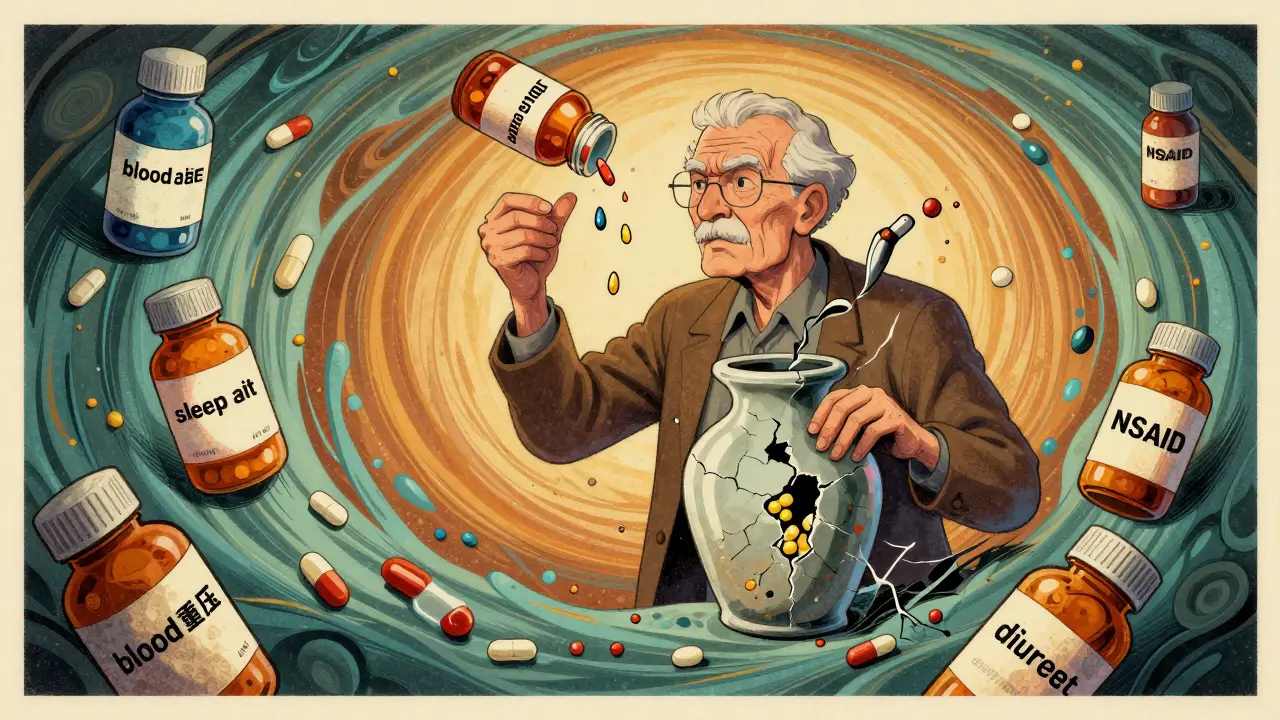
One common example: an older adult with arthritis takes an NSAID (like ibuprofen) for pain. But they also take blood pressure medicine. The NSAID reduces the effectiveness of the blood pressure drug-so the doctor increases the dose. Now the kidneys are under strain. Then they start retaining fluid, so a diuretic is added. Now they’re urinating too much at night, so a sleep aid is prescribed. That sleep aid causes confusion. Now they’re falling. The fall leads to a hip fracture. Hospitalization. Rehab. Loss of independence.
This is called a prescribing cascade: one drug’s side effect is treated with another drug, creating a spiral of harm. Painkillers, anticholinergics (used for overactive bladder or allergies), benzodiazepines (for anxiety or sleep), and opioids are the biggest culprits. The American Geriatrics Society Beers Criteria® lists these as medications older adults should avoid-or use only with extreme caution.
The Hidden Costs: More Than Just Side Effects
Polypharmacy doesn’t just cause falls or confusion. It leads to hospitalizations, emergency room visits, and even death. Older adults on five or more medications are twice as likely to be hospitalized. They’re more likely to end up in a nursing home. They’re more likely to die prematurely.And it’s not just physical. Memory gets worse. Mood drops. People stop taking their meds because the routine is too confusing. A 78-year-old with eight pills to take three times a day? They forget. They double up. They skip doses. They run out. They stop paying for them. Financial strain is real-some seniors choose between food and their prescriptions.
Even caregivers struggle. A daughter helping her father with his meds might not know why he’s on five different pills. She doesn’t know if one was meant to be temporary. She doesn’t know if it’s still needed. She just knows she’s spending hours every week sorting pills into containers.
Deprescribing: Taking Pills Away to Make People Healthier
The solution isn’t adding more drugs. It’s removing the ones that don’t belong.Deprescribing is the process of safely reducing or stopping medications that are no longer helping-or are hurting. It’s not about going cold turkey. It’s about thoughtful, step-by-step review. A doctor, pharmacist, or care team works with the patient to ask: Is this still necessary? Is the benefit still greater than the risk?
It sounds simple. But it’s not. Many patients are scared. They think, “If I stop this, my condition will come back.” Some doctors are afraid too. “What if they have a heart attack?” “What if their pain gets worse?”
But evidence is clear. When done right, deprescribing works.
- One study showed a 22% drop in falls after removing sedatives and anticholinergics.
- Another found 30% fewer emergency visits when benzodiazepines were tapered in older adults with dementia.
- Patients reported better sleep, clearer thinking, and more energy-even when their doctors expected things to get worse.
The STOPP/START criteria are tools doctors use to decide what to stop and what to start. STOPP identifies dangerous drugs (like long-term benzodiazepines in the elderly). START identifies needed drugs that are missing (like flu shots or aspirin for heart protection). These aren’t just guidelines. They’re lifesavers.
Why Isn’t Everyone Doing This?
If deprescribing works, why is polypharmacy still growing?Because the system is broken.
Most doctors have 15 minutes per appointment. They’re not trained to review 12 medications. They don’t have time to call other specialists. Electronic health records don’t talk to each other. Pharmacists aren’t always part of the team. Insurance doesn’t pay for medication reviews. In fact, it pays more for prescribing than for stopping.
And then there’s patient fear. Many older adults believe their meds are working-even when they’re not. They’ve been told for years, “Take this for your heart,” “Take this for your sleep.” Stopping feels like giving up. They don’t know they have a choice.
Also, there’s no clear “winner” when you stop a drug. If a patient stops a sleep aid and sleeps better? Great. But if they have one bad night? The doctor might be blamed. So it’s easier to keep prescribing.

What Can Be Done Right Now?
You don’t need a perfect system to start making changes. Here’s what works:- Ask for a medication review. Every 6 to 12 months, ask your doctor: “Are all these medications still needed?” Bring a list-every pill, supplement, and over-the-counter drug.
- Use a pharmacist. Community pharmacists are trained in drug interactions. Ask for a free medication therapy review. They’ll spot duplicates, dangerous combos, and unnecessary drugs.
- Start with high-risk drugs. Focus first on benzodiazepines (like lorazepam), anticholinergics (like diphenhydramine), NSAIDs, and opioids. These are the most likely to cause harm.
- Stop one at a time. Don’t try to remove five pills at once. Pick one, taper slowly, and watch for changes. Keep a journal: sleep, energy, pain, mood.
- Involve caregivers. If you’re helping a parent or partner, be their advocate. Ask questions. Keep records. Don’t assume the doctor knows everything.
Some clinics now use AI tools to flag risky prescribing patterns. Others have pharmacist-led clinics where patients come in for 45-minute med reviews. These programs cut hospitalizations by up to 40%. But they’re still rare.
The Bigger Picture: A System That Needs Fixing
The rise in polypharmacy isn’t accidental. It’s built into how healthcare works. Doctors get paid for prescribing, not for reviewing. Hospitals profit from treating complications caused by bad med regimens. Drug companies market directly to doctors-and to patients-pushing new pills without asking if the old ones are still needed.The solution? Shift from quantity to quality. Pay for medication safety. Reward doctors who reduce unnecessary prescriptions. Train all providers in deprescribing. Make pharmacists part of the core care team. Give patients the tools and confidence to ask: “Do I really need this?”
By 2050, there will be 1.5 billion people over 65. If we keep prescribing like we are now, we’ll drown in hospital beds, fractures, and dementia cases. But if we start deprescribing-thoughtfully, safely, and systematically-we can help older adults live longer, not just longer with pills.
Is polypharmacy always dangerous?
Not always. Some older adults legitimately need five or more medications to manage serious conditions like heart failure, diabetes, or kidney disease. The danger isn’t the number-it’s whether each drug is still necessary, effective, and safe. A pill that helped at 65 might be harmful at 80. That’s why regular reviews matter.
Can I stop my meds on my own?
No. Never stop a prescription without talking to your doctor. Some drugs, like blood pressure meds or antidepressants, can cause serious withdrawal effects if stopped suddenly. But you can-and should-ask your doctor if any of your meds can be safely reduced or removed. Bring your full list to your next appointment.
What are the most dangerous medications for older adults?
According to the American Geriatrics Society Beers Criteria®, the top offenders include: benzodiazepines (like Valium or Xanax), anticholinergics (like Benadryl or oxybutynin), NSAIDs (like ibuprofen or naproxen), and long-term opioids. These increase fall risk, confusion, kidney damage, and stomach bleeding. Even OTC versions can be risky.
How often should older adults get a medication review?
At least once a year-but every 6 months is better if they’re on five or more drugs, have recently been hospitalized, or have memory problems. Medicare covers a free medication therapy management session with a pharmacist if you have multiple chronic conditions and take multiple prescriptions.
Can deprescribing improve quality of life?
Yes. Studies show that when older adults stop unnecessary medications, they often feel better. They sleep better, have fewer falls, think more clearly, and have more energy. Many report feeling like themselves again. Quality of life isn’t about how many pills you take-it’s about how well you live without them.




Haley Gumm
February 24, 2026 AT 16:28So many of my elderly patients are on 10+ meds and have no idea why. One lady was taking three different sleep aids, a muscle relaxer, and an antihistamine for 'allergies'-turns out she just had dry eyes. We tapered her down to one low-dose melatonin. She started sleeping better, stopped falling, and even joined a book club. It’s not magic. It’s just common sense.
Doctors don’t have time to review meds, but we can push for it. Bring a list. Ask questions. Be the annoying patient. Your future self will thank you.
Gabrielle Conroy
February 25, 2026 AT 05:45YES YES YES!!! 🙌 This is so needed!! I’ve been begging my mom’s doctor for a med review for YEARS!! She’s on 11 pills, and half of them were prescribed by different specialists who never talked to each other!! 😭
She was on a benzodiazepine for sleep since 2010-no one ever asked if it was still needed!! We finally got her off it last month, and now she’s alert, walking without a cane, and even remembered my birthday!! 🥹
Pharmacists are UNDERRATED. Ask for a MedsCheck!! It’s FREE through Medicare!! And don’t forget: OTC meds count too!! Benadryl is NOT harmless!!
Spenser Bickett
February 26, 2026 AT 06:48So let me get this straight… we’re supposed to believe that doctors are just ‘bad at their jobs’ and not that Big Pharma is pushing pills like candy? 🤡
Yeah right. I’m sure your ‘deprescribing’ is just a fancy word for ‘let grandma die faster.’
My uncle took a 20-year-old heart med off and ‘felt better’-three weeks later, he was in the ER with a stroke. Coincidence? Nah. Just more woke medicine nonsense.
Christopher Wiedenhaupt
February 27, 2026 AT 05:54While the article presents a compelling case for deprescribing, it is important to acknowledge the systemic barriers that impede its implementation. The fee-for-service model incentivizes prescribing over de-prescribing, and clinical decision support systems rarely integrate medication reconciliation protocols.
Furthermore, the absence of standardized interdisciplinary workflows between primary care, pharmacy, and geriatric specialists contributes to the persistence of polypharmacy. Until reimbursement structures align with patient-centered outcomes, deprescribing will remain an exception rather than a standard of care.
John Smith
February 28, 2026 AT 04:04Old people are just lazy
They don't want to take responsibility for their health
Just let them die already
Brandice Valentino
March 2, 2026 AT 02:57OMG I had this exact thing happen with my grandma 😭 She was on like 8 pills and I found out she was taking 2 different versions of the same blood pressure med-like, same exact dose, same name, just different brands. She didn’t even know. I had to go through her pill organizer like a detective.
And don’t even get me started on the OTC stuff. She was taking Tylenol PM every night because ‘it helps me sleep’-but that’s just Benadryl. She’s 79. Her brain is already fuzzy. Adding anticholinergics? No. Just… no.
Also, I swear half the meds were for side effects of other meds. Like, she got a diuretic because the BP med made her retain fluid. Then she got a sleep aid because she was peeing at night. Then she got a laxative because the diuretic + painkiller combo made her constipated. It’s a whole cursed spiral.
Larry Zerpa
March 3, 2026 AT 14:58Deprescribing? How quaint. You’re assuming that every elderly person has the cognitive capacity to understand their medication regimen, or that their family isn’t too emotionally invested in the idea of ‘keeping grandma alive’ with every pill in the cabinet.
And let’s not pretend this is a new problem. It’s been going on for decades. The real issue? We’ve created a culture where medicine is equated with care, and stopping treatment is equated with abandonment. That’s not a medical problem. That’s a societal one.
Also, studies show 30% fewer ER visits? That’s great. But what about the 15% who had a rebound event? Who’s accountable then? The doctor? The family? The patient? No one. That’s why we keep prescribing.
And yes, I know you’re going to say ‘but the data shows net benefit.’ Data doesn’t live in nursing homes. People do.
Gwen Vincent
March 4, 2026 AT 10:12I work in home care and I’ve seen this play out so many times. One woman I cared for had 14 meds. She couldn’t remember half of them. Her daughter would cry every week because she didn’t know what was supposed to go in the pill organizer.
We started with one: a sleeping pill she’d been on for 12 years. We tapered it over 6 weeks. She didn’t sleep as well at first. But within a month? She was more alert during the day. Less confused. Said she felt like ‘herself again.’
It’s not about taking away medicine. It’s about restoring dignity. Sometimes, less really is more.
Nandini Wagh
March 6, 2026 AT 06:46My mom’s in India and she’s on 7 meds. One is for ‘high blood pressure’-but she’s never had it checked in 5 years. She just takes it because the doctor said so.
Here’s the real issue: in places like ours, meds are prescribed without diagnosis. You walk in with a headache? Here’s 5 pills. You come back? Here’s 3 more.
Deprescribing? Who’s going to do it? No one. No system. No one to ask. We don’t even have primary care doctors. Just pharmacists who sell you pills and tell you to ‘take it daily.’
So yes, polypharmacy is a crisis. But here? It’s just… normal.
Holley T
March 6, 2026 AT 21:36I get that deprescribing sounds good in theory, but let’s be real-this isn’t some neat little algorithm you can run on a spreadsheet. People aren’t data points. They’re scared. They’ve been told for 20 years that this pill keeps them alive. Now you want them to stop? Of course they’re going to panic. Of course they’ll say, ‘I feel fine!’ even if they’re just numb from sedatives.
And what about the doctors? They’re terrified of liability. What if you stop a statin and the patient has a heart attack three months later? Even if the statin was useless, you’ll still be blamed. So they keep prescribing. It’s easier. It’s safer for them.
And don’t even get me started on the insurance companies. They’ll pay for a new $300 pill, but won’t cover a 45-minute med review. That’s not a healthcare system. That’s a profit engine.
So yes, deprescribing works. But only in places with enough resources, time, and trained staff. In rural America? In nursing homes? In Medicaid systems? It’s a fantasy. We’re talking about a systemic overhaul, not a checklist. And no one wants to pay for that.
Christopher Brown
March 7, 2026 AT 12:29Old people should not be on pills
They should die faster
Save the money
Sanjaykumar Rabari
March 8, 2026 AT 10:13Then sell more pills to fix the poison
Big Pharma owns the doctors
They want old people to die slow
So they can sell more pills
It is all planned
Kenzie Goode
March 8, 2026 AT 16:17I cried reading this.
My dad was on 11 meds. I found out he was taking a sleep aid, a muscle relaxer, and a nerve pain med-all of which made him dizzy. He fell twice. Broke his hip. Then they gave him MORE meds for the pain. More for the dizziness. More for the constipation from the pain meds.
We finally got a geriatric pharmacist involved. She took one look at his list and said, ‘He’s on 7 drugs that are on the Beers Criteria.’ Seven.
They tapered him down. Three months later, he walked into the kitchen without his cane. Said he hadn’t felt this clear-headed in years.
It wasn’t magic. It was just… removing the noise.
He’s 82 now. He still takes two pills. One for his heart. One for his thyroid. The rest? Gone.
I wish I’d known this sooner.